Process Mining in Healthcare: A Systematic Literature Review and A Case Study
 , Chiara Colucci 2, Angelo Corallo 1, Roberto Paiano 1, Claudio Pascarelli 1
, Chiara Colucci 2, Angelo Corallo 1, Roberto Paiano 1, Claudio Pascarelli 1
Adv. Sci. Technol. Eng. Syst. J. 7(6), 151–160 (2022);
 DOI: 10.25046/aj070615
DOI: 10.25046/aj070615
Process mining is an innovative technique through which inefficiencies in production systems can be eliminated. This technique has therefore become very important internationally in recent years and is also useful for pursuing the improvement of production systems by extrapolating process knowledge from event logs recorded by information systems. Process mining has easy application in production systems as current business processes are integrated with information systems and this makes data available immediately. This makes the complex nature of industrial operations understandable and, for this reason, process mining could also be used in the healthcare field where cost containment and the quality of service increasing offered to the community has become paramount. The problem is that in this sector, it is much more complex to identify useful data in order to extrapolate the relevant log file. The article aim is to examine the state of the art of the application of process mining in the healthcare sector in order to understand the level of diffusion of these techniques. In the light of this analysis, a case study will then be analysed on the application of process mining techniques in the healthcare sector, and in particular in medical teleconsultation in the field of neuroradiology.
1. Introduction
This paper is an extension of the work originally presented in “Application of Process Mining in Teleconsultation Healthcare: Case study of Puglia Hospital” [1].
Process mining is a recently applied research discipline which combines data mining and computational intelligence on the one hand with process analysis and modelling on the other [2], [3].
Despite the relative youth of this discipline, many techniques and methodologies have been implemented. The most widely used are: Fuzzy and Heuristic Miner. The first algorithm allows the process model to be made simpler, as this technique reduces the model to a desired abstraction threshold and is, therefore, particularly suitable for the extraction of less structured processes with a large amount of conflicting behaviour [4]. The second uses frequencies and parameterisation so that the main behaviour can be recorded in an event log. Considering the dependency measure, it takes into account frequencies and causal dependencies, making it suitable for many real logs [5].
In particular, process mining involves the discovery of processes, the monitoring of compliance through the analysis of deviations (which can be either negative or positive) from best practices and the optimisation of the model based on the deviations found.
Indeed, process mining was born with the aim of extracting knowledge from current information systems (using event logs that can be easily accessed), and through this, to be able to discover, monitor and improve real processes [6]. This technique consists of three phases:
1) discovery (process models are extracted from an event log);
2) conformance checking (or check of any deviation between the model and the log by making a comparison);
3) enhancement (using the information in the logs, improves or extends a process model) [7].
Consequently, the application of these techniques is particularly useful in industrial scenarios where there is the production of complex goods, and, therefore, the analysis of a large amount of information becomes necessary for the development management of new applications.
Another natural application field of process mining analysis is healthcare [8], [9]. Several case studies exist in which process mining techniques and tools are applied in this sector [10], [11]. Among these, the oncology and the hospitalisation sector show the maximum number of successful cases [12]. Hospitals, for example, need to focus on managing their processes to have high quality services while reducing costs, especially when patient demand unexpectedly increases (as was the case with the COVID-19 pandemic crisis) [13]-[15]. The biggest problem in the healthcare sector is that the patient care process (“care flow”) very often differs even if the patients have a similar diagnosis. The techniques under consideration offer an interesting possibility through which this problem can be solved: process mining has already been used to a very significant extent in service companies and could therefore also be a good solution in the health sector [16], [17].
Another problem is the existence of several systems which store events and data. An intensive care unit, for example, is very often equipped with its own system to store patients’ treatments or examinations, while the radiology department has another system to store the entire patient process. It becomes, therefore, crucial that all information is amalgamated in a single source. However, given the great multiplicity of systems involved, which makes data collection complex, process mining techniques could prove very useful as they would allow, starting from the individual events carried out in each division, to obtain the entire process, which could provide an overview that, for example, could ensure good reporting of the examinations performed [18], [19].
In this paper, the first two sections we introduce, explain and give a systematic literature review which evaluates the process mining tools applications in the healthcare scenario. According to its definition, a systematic literature review is “A review of a clearly formulated question that uses systematic and explicit methods to identify, select, and critically appraise relevant research, and to collect and analyse data from the studies that are included in the review. Statistical methods (meta-analysis) may or may not be used to analyse and summarise the results of the included studies” [20].
With this systematic search process, we identify studies addressing a specific research question and we make a systematic presentation and synthesis of the characteristics and outcomes of the research findings. The criteria by which studies are excluded or included are objective, consistently applied and explicitly stated, so that when certain studies are included or excluded from the review, this decision is clear to the readers; or if another researcher decides to use the same criteria, he or she is likely to replicate the same decisions [21].
In the second section we present the Tranfield approach that is used to conduct the systematic literature review, allowing the identification of the most interesting documents in the analysed context. In the third section we show up our case study: an analysis of the log file extracted from the Apulian hospitals’ repository. In section 4, we illustrate the use of process mining techniques on the log file (using Disco software [22]) and analyse the results achieved with these techniques. Then, in this section, the AS-IS process is represented with BPMN notation (using the Signavio tool). In the last section, the results of our case study are compared with data related to the Piedmont Region (representing a virtuous Italian region), which are taken from the official source of the Ministry of Health. At this point, we modelled a TO-BE process to optimise the current process.
Finally, there are our conclusions and the references used. Ultimately, our analysis aim is not to investigate new issues but, based on the state of the art, to highlight that Process Mining techniques are useful in healthcare applications. From the above, we can extrapolate the following research question:
“RQ – Provided the state of the art obtained from the SLR, and aimed at identifying the scope of application in healthcare, does the use of teleconsultation optimise the performance of the healthcare service in the field of neuroradiology?”
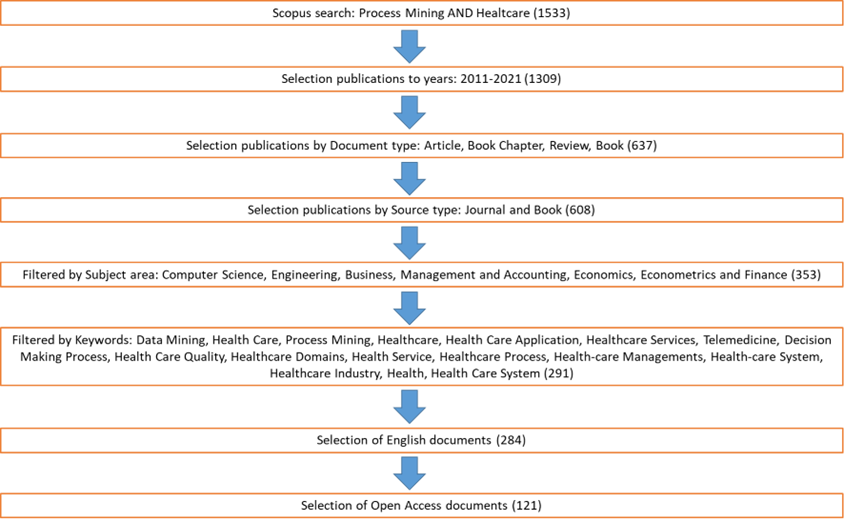
Figure 1 – The process of systematic literature review
2. Research Method
Since this is a review article, we will now apply the Tranfield approach to conduct a systematic literature review (SLR), finalised to highlight the usefulness of Process Mining techniques in healthcare applications.
In clinical disciplines, the method theorised by Egger [23] is used to implement a systematic review (SR). We apply the Tranfield approach to develop the “Study Selection” phase of Egger’s method, a phase through which the various studies identified are evaluated, so that it is possible to assess whether or not the inclusion criteria are met. The Tranfield approach uses three phases: planning, execution, reporting and dissemination.
In the planning phase, we enter the terms “Process mining” AND “Healthcare” to search for the keywords, abstract and title. Starting to execution, the initial Scopus search, (we are selected the Scopus database to guarantee the review’s quality) on the basis of the selected words present in keywords, abstract and title, found a total of 1533 publications. Then, we are limited the analysis to the last 11 years (2011–2021), as our research interest is based on these years, resulting in 1309 publications [21].
By restricting the search to “Article”, “Book chapter”, “Review”, and “Book”, we found a total of 637 publications. Considering only the publications in Journals and Books, we identified 608 documents. However, to achieve the aims set initially, we selected only documents included in the fields of Computer Science, Engineering, Business, Management and Accounting, Economics, Econometrics and Finance finding a total of 353 publications.
The selected fields are the one of interest which refer to the case study analysed in the paper. In fact, as mentioned before in the RQ, the aim is to analyse the impact of teleconsultation from a technical point of view (hence the choice of the fields “Computer Science” and “Engineering”), and from a monetary point of view (hence the choice of the fields “Business, Management and Accounting”, “Economics, Econometrics and Finance”). At this point, given the important number of articles found, and considering that the ones of greatest interest would be those incorporating the keywords, we applied a new filter (the keywords selected were: “Data Mining”, “Health Care”, “Process Mining”, “Healthcare”, “Health Care Application”, “Healthcare Services”, “Telemedicine”, “Decision Making Process”, “Health Care Quality”, “Healthcare Domains”, “Health Service”, “Healthcare Process”, “Health-care Managements”, “Health-care System”, “Healthcare Industry”, “Health”, “Health Care System”), obtaining 291 publications. After choosing the English language (284), and the Open Access documents, we found 121 documents. Figure 1 shows the SLR process. Finally, we faced the last phase of the Tranfield approach, namely reporting and dissemination.
As we show in Figure 2, the number of publications has increased in the last three years: 14 in 2019, 22 in 2020, 26 in 2021. In the previous years, there was an average of 6 publications, with a marked increase in 2018 (21 publications).
This trend highlights the growing attention to these topics in recent years. In addition, 65 journals published the topics analysed, 11 out of which published two or more articles (59), representing 49% of the total. Analysing the Scopus impact evaluation of sources with most publications, 78% were in the first quartile (which represents the highest quality of the publication magazine); 15% in the second; and only 7% in the third, demonstrating the high standard of the publications, and the level of interest in the subjects (Table 1 and Figure 3) [24], [25].
Figure 2 – Documents by year. Source: Scopus
Table 1 – Journals with two or more documents published
| Source | Documents | Ranking Scopus |
| “IEEE Access” | 21 | Q1 |
| “Journal of Biomedical Informatics” | 13 | Q1 |
| “IEEE Journal of Biomedical and Health Informatics” | 4 | Q1 |
| “International Journal of Advanced Computer Science and Applications” | 4 | Q3 |
| Sensors (Switzerland) | 4 | Q2 |
| Applied Sciences (Switzerland) | 3 | Q2 |
| Artificial Intelligence in Medicine | 2 | Q1 |
| Computers Materials and Continua | 2 | Q1 |
| Expert Systems with Applications | 2 | Q1 |
| Plos Computational Biology | 2 | Q1 |
| Sensors | 2 | Q2 |
| Other | 62 | |
| Total | 121 |
Figure 3 – Documents per year by source. Source: Scopus
Moreover, we observed an increase in the number of publications for IEEE Access Journal (Q1) in the years 2018, 2019 and 2020, from 4 in 2018 to 7 in 2020, which again reflects the increasing interest in these themes in recent years.
The Affiliation Identifier allows us to identify and distinguish publications in relation to the reference institutions or organizations. In this case, we noted that the majority of publications comes from the Education area (University, Institute, Laboratory, School, College), followed by other areas: Company, Health Management, Research and Government (Figure 4)
Figure 4 – Documents by affiliation. Source: Scopus
Figure 5 – Documents by country or territory. Source: Scopus
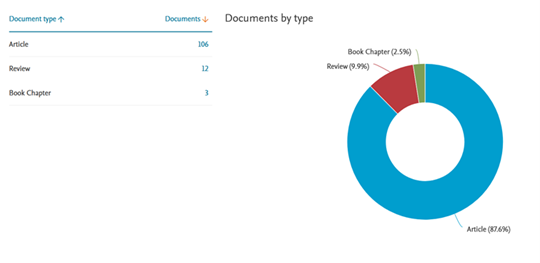
Figure 6: Documents by type. Source: Scopus
Another interesting aspect is the publications on the analysed topics by countries. In particular, most publications were produced in Asian territories (China and Middle East), followed by Europe (United Kingdom, France, Netherlands, Italy), and finally by America (principally United States). This may be further incentive to increase publications in our area (Figure 5).
Figure 7: Documents by Subject area (Source: Scopus)
Moreover, as shown in Figure 6, publications consisted mainly of articles (106 – 87,6%), and some reviews (12 – 9,9%). In line with the selected Subject areas for the SLR, the majority of publications were in the Computer Science (110 – 34%) and Engineering (61 – 19%) areas. The areas “Business, Management and Accounting” and “Economics, Econometrics and Finance” counted 13 (4%), and 4 (1%) publications respectively (Figure 7). These findings shows that process mining applied to the healthcare sector has become very useful and relevant [26]. In particular, of the 27 papers about Medicine, the majority (17 – (63%)) concerned research activities in the field of healthcare using innovative approaches, such as: Health Surveillance Software Framework, Time Series Data Mining, Electronic Medical Record Search Engine, Intelligent Personal Health Record. Part of them regarded studies and applications of process mining in the field of neurological pathologies (2 – (7%)), cardiological pathologies (2 – (7%)), and in the radiology sector (2 – (7%)). In the remaining part of this sample, the authors discussed application cases on psychiatric diseases, diabetes and cancer. Since the review process we carried out have not delivered any paper on medical teleconsultation analysis in the neuroradiology field, in this paper we decided to analyse a case study on this subject. This case study is presented in the following section.
3. Case study
Following the considerations in the previous section, in this one we show the case study based on an analysis of process mining about clinical teleconsultation in the neuroradiology domain. We choose the teleconsultation as main topic, since it represents a new and innovative approach to healthcare delivery, also in the light of the pandemic period, therefore representing a very actual topic. Within the scope of this paper, we imagine the process as follows: after the patient is admitted to a medical district, the referring physician requires certain analysis and exams. Once all the necessary documents have been provided, the corresponding doctor sends all the documents (results of tests, images and diagnosis [if expressed]) to the specialist doctor for a second opinion. The specialised doctor returns his/her own diagnosis with the corresponding treatment or further examinations. At this stage, the patient must undergo the suggested treatment until discharge.
The file log represented in the Table 2 derives from this repository. This log file represents the effective process, knowing that we have anonymised the patient and doctor data. For simplicity, we report only two cases and we add a cost column to the extracted data. The costs presented are the real ones for each activity with the exception of the activity “blood test”. For the latter, in fact, we used a flat-rate cost, as a result of ten examinations usually carried out in the medical field of reference, at the cost of 10 euros on average.
After acceptance, the patient is assigned to the referring doctor (the corresponding doctor). The physician, after visiting the patient and submitting him or her to the appropriate examinations, analyses the patient’s medical history and, if he or she considers it appropriate, may request the specialist support for a second opinion. To request the specialist’s support, the physician uses the teleconsultation tool and sends all the documents to the specialised doctor.
When the documentation received has been examined, the specialist can send the diagnosis to the applicant or request further examinations. After the diagnosis has been expressed, the patient must follow the suggested treatment before discharge (patient 1) or is directly discharged if no specific problems occur (patient 2).
In next section we will use this log file to obtain the real process.
Table 2 – Log file of process
| Case id
(patient) |
Event identification | Timestamp | Activities | Resource | Price (€) |
| A | 1 | 12/05/2020 h. 08:30 | Patient acceptance | Reception | 26,40 |
| A | 2 | 14/05/2020 h. 10:30 | Referral to the requesting doctor | Support Service | 26,51 |
| A | 3 | 17/05/2020 h. 09:30 | Visit schedule | Support Service | 26,50 |
| A | 4 | 08/06/2020 h. 09:30 | Patient official visit | Doctor Silver
(Corresponding doctor) |
36,16 |
| A | 5 | 10/06/2020 h. 11:00 | Angio exam | Doctor Coral | 313,19 |
| A | 6 | 11/06/2020 h. 09:30 | MRI (Magnetic Resonance Imaging) | Doctor Beige | 46,14 |
| A | 7 | 11/06/2020 h. 12:30 | Blood analysis | Doctor Blue | 80,00 |
| A | 8 | 13/06/2020 h. 10:15 | Visit schedule | Support service | 26,51 |
| A | 9 | 01/07/2020 h. 15:30 | Patient official visit | Doctor Silver | 36,15 |
| A | 10 | 04/07/2020 h. 14:00 | Request of teleconsultation | Doctor Silver | 25,83 |
| A | 11 | 05/07/2020 h. 11:00 | Evaluation of the request for consultation | Doctor Golden (Specialised doctor) | 41,32 |
| A | 12 | 06/07/2020 h. 12:30 | Specialist diagnosis sending | Doctor Golden | 33,56 |
| A | 13 | 08/07/2020 h. 13:30 | Visit schedule | Support service | 26,50 |
| A | 14 | 18/07/2020 h. 15:30 | Patient official visit | Doctor Silver | 36,17 |
| A | 15 | 29/07/2020 h. 13:15 | Radiation therapy I cycle | Doctor Magenta | 987,81 |
| A | 16 | 10/08/2020 h. 08:30 | Blood analysis | Doctor Blue | 80,00 |
| A | 17 | 16/08/2020 h. 10:30 | Radiation therapy II cycle | Doctor Magenta | 987,80 |
| A | 18 | 18/08/2020 h. 08:30 | Blood analysis | Doctor Blue | 80,00 |
| A | 19 | 21/08/2020 h. 10:30 | Radiation therapy III cycle | Doctor Magenta | 987,81 |
| A | 20 | 23/08/2020 h. 08:30 | Blood analysis | Doctor Blue | 80,00 |
| A | 21 | 25/08/2020 h. 09:15 | Visit schedule | Support Service | 26,51 |
| A | 22 | 10/09/2020 h. 12:00 | Patient official visit | Doctor Silver | 36,16 |
| A | 23 | 12/07/2020 h. 09:00 | Patient discharge | Reception | 26,40 |
| B | 24 | 06/06/2020 h. 10:00 | Patient acceptance | Reception | 26,40 |
| B | 25 | 10/06/2020 h. 12:15 | Referral to the requesting doctor | Support Service | 26,51 |
| B | 26 | 12/06/2020 h. 13:00 | Visit schedule | Support Service | 26,50 |
| B | 27 | 05/07/2020 h. 11:30 | Patient official visit | Doctor Brown
(Corresponding doctor) |
36,16 |
| B | 28 | 08/07/2020 h. 13:30 | Eco-doppler exam | Doctor Coral | 80,00 |
| B | 29 | 10/07/2020 h. 12:00 | Blood analysis | Doctor Blue | 80,00 |
| B | 30 | 13/07/2020 h. 13:00 | CT (Computed Tomography) scanning | Doctor Blue | 56,15 |
| B | 31 | 15/07/2020 h. 12:20 | Visit schedule | Support Service | 26,50 |
| B | 32 | 28/07/2020 h. 15:00 | Patient official visit | Doctor Brown | 36,16 |
| B | 33 | 06/08/2020 h. 13:00 | Request of teleconsultation | Doctor Brown | 25,82 |
| B | 34 | 07/08/2020 h. 07:00 | Evaluation of the request for consultation | Doctor Lime (Specialised doctor) | 41,32 |
| B | 35 | 09/08/2020 h. 08:15 | Sending the request for a new test to the Specialist | Doctor Lime | 33,54 |
| B | 36 | 11/08/2020 h. 07:00 | Patient communication | Support Service | 26,50 |
| B | 37 | 14/08/2020 h. 10:00 | PET (Positron Emission Tomography) exam | Doctor Azure | 42,21 |
| B | 38 | 16/08/2020 h. 08:40 | Visit schedule | Support Service | 26,50 |
| B | 39 | 25/08/2020 h. 12:15 | Patient official visit | Doctor Brown | 36,15 |
| B | 40 | 05/09/2020 h. 09:00 | Request of teleconsultation | Doctor Brown | 25,82 |
| B | 41 | 06/09/2020 h. 08:15 | Evaluation of the request for consultation | Doctor Lime | 41,33 |
| B | 42 | 08/09/2020 h. 15:15 | Specialist diagnosis sending | Doctor Lime | 33,56 |
| B | 43 | 10/09/2020 h. 09:10 | Visit schedule | Support Service | 26,50 |
| B | 44 | 25/09/2020 h. 17:00 | Patient official visit | Doctor Brown | 36,17 |
| B | 45 | 26/09/2020 h. 07:30 | Patient discharge | Reception | 26,40 |
(Source: own elaborations)
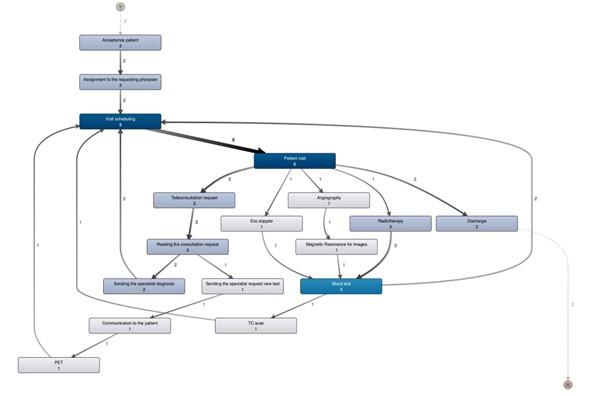
Figure 8: Process discovered (Source: own elaborations)
4. Process mining application and results
In this paragraph we perform the discovery process as the first step using the Disco software. Elaborating the log file with this software we deliver the process shown in Figure 8.
As we can see, the process obtained from this application does not lead to a good performance. It presents bottlenecks, and even when the teleconsultation tool is used, the case duration is still high.
In particular, the bottlenecks are related to the following resources: Reservation centre (24,44%), Visit scheduling (17,78%), Patient visit (17,78%). Presenting a higher utilisation rate than the other resources, which instead present an underutilised capacity, the above-listed resources led to the entire process slowdown.
Table 3 – Statistics for case
| Case id | Event | Length | Price | Event price |
| A | 23 | 118 days | 4.073,39 | 117,10 |
| B | 22 | 104 days 30 minutes | 816,22 | 37,10 |
| Tot. | 45 | 4.889,61 | 154,20 |
This aspect is more evident in the following data (Table 3, Table 4 and Table 5).
Now, we use the Business Process Management (BPM) approach in order to model, define, organize and monitor the healthcare processes, analysing and consequently optimising the clinical activities under study [27]. For the graphical representation of process steps, we have adopted the Business Process Model and Notation (BPMN) [28], [29].
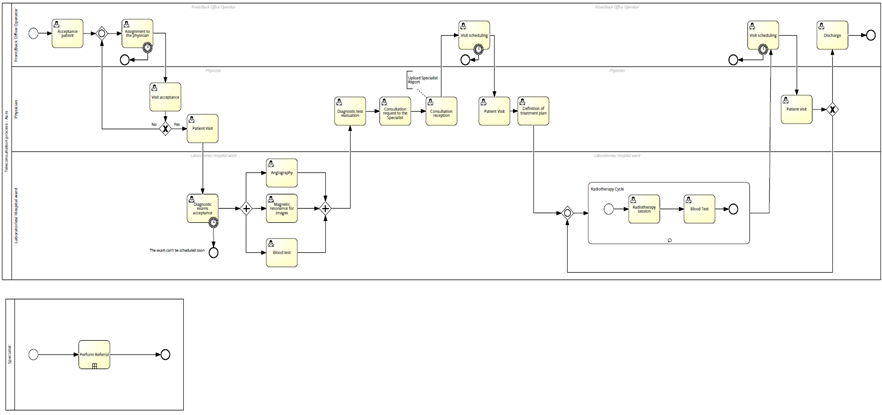
Figure 9 – AS-IS process
Table 4 – Statistics for activity
| n. | Activity | % | Freq. |
| I | Visit schedule | 17,78% | 8 |
| II | Patient official visit | 17,78% | 8 |
| III | Blood analysis | 11,11% | 5 |
| IV | Request of teleconsultation | 6,67% | 3 |
| V | Evaluation of the request for consultation | 6,67% | 3 |
| VI | Radiation therapy | 6,67% | 3 |
| VII | Patient acceptance | 4,44% | 2 |
| VIII | Referral to the requesting doctor | 4,44% | 2 |
| IX | Specialist diagnosis sending | 4,44% | 2 |
| X | Patient discharge | 4,44% | 2 |
| XI | Angio exam | 2,22% | 1 |
| XII | MRI (Magnetic Resonance Imaging) | 2,22% | 1 |
| XIII | Eco-doppler exam | 2,22% | 1 |
| XIV | CT (Computed Tomography) scanning | 2,22% | 1 |
| XV | Sending the request for a new test to the Specialist | 2,22% | 1 |
| XVI | Patient communication | 2,22% | 1 |
| XVII | PET (Positron Emission Tomography) exam | 2,22% | 1 |
| Tot. | 100,00% | 45 |
Table 5 – Statistics for resource
| n. | Resource | % | Freq. |
| I | Support Service | 24,44% | 11 |
| II | Doctor Blue | 13,33% | 6 |
| III | Doctor Brown | 13,33% | 6 |
| IV | Doctor Silver | 11,11% | 5 |
| V | Reception | 8,89% | 4 |
| VI | Doctor Lime | 8,89% | 4 |
| VII | Doctor Magenta | 6,67% | 3 |
| VIII | Doctor Coral | 4,44% | 2 |
| IX | Doctor Golden | 4,44% | 2 |
| X | Doctor Beige | 2,22% | 1 |
| XI | Doctor Azure | 2,22% | 1 |
| Tot. | 100,00% | 45 |
In particular, the process flow modelled with BPMN notation [30] using Signavio tool is visible in the following figure (Figure 9):
5. Discussion
Starting from the results presented in the previous section, it emerges that our application reveals a fundamentally non-performing process. The analysis actually showed that the process is very slow (almost three months in both cases described), and there are bottlenecks in both resource and activities utilisation.
Then, we match the adopted practices with the best practices implemented in Piedmont, considered a virtuous region. The log file of Piedmont was not available, and therefore we were not possible to perform a compliance between the two processes. From observing data from the Ministry of Health (Table 6), the number of test equipment in Apulia was much lower, and this create bottlenecks, since many more tests are needed in Apulia than in Piedmont. Furthermore, from the same statistics, we realize that the number of personnel employed in Piedmont was higher than in Apulia, and this affected the unitary personnel performance which, therefore, is higher in Apulia than in Piedmont. This leads to an over- utilisation of the units of work, and consequently bottlenecks also in terms of care pathway duration. These aspects are highlighted in Table 6.
Table 6: Data
| Category | Classification | Region | Value |
| Medical devices number | Angio exam
|
Region 1
Region 2 |
31
12 |
| MRI (Magnetic Resonance Imaging) | Region 1
Region 2 |
33
16 |
|
| Eco-doppler exam | Region 1
Region 2 |
364
138 |
|
| PET (Positron Emission Tomography) exam | Region 1
Region 2 |
2
0 |
|
| CT (Computed Tomography) scanning | Region 1
Region 2 |
80
49 |
|
| Medical devices performance (per number) | Eco-doppler exam | Region 1
Region 2 |
1646,8
2818,2 |
| CT (Computed Tomography) scanning | Region 1
Region 2 |
3960,0
3986,9 |
|
| MRI (Magnetic Resonance Imaging) | Region 1
Region 2 |
2041,3
2694,4 |
|
| Age of devices (%) | > 15 years | Region 1
Region 2 |
6,5%
18,3% |
| 10-15 years | Region 1
Region 2 |
20,7%
16,6% |
|
| 10-7 years | Region 1
Region 2 |
13,7%
19,1% |
|
| 7-3 years | Region 1
Region 2 |
23,5%
18,0% |
|
| < 3 years | Region 1
Region 2 |
35,7%
28,0% |
|
|
Staff workload |
Performance per staff unit | Region 1
Region 2 |
1362
1647 |
| Performance by technician | Region 1
Region 2 |
2648
3114 |
|
| Performance by physician | Region 1
Region 2 |
5800
6215 |
|
|
Operating personnel |
Facility managers | Region 1
Region 2 |
107
60 |
| Medical managers | Region 1
Region 2 |
507
271 |
|
| Physical | Region 1
Region 2 |
47
12 |
|
| Radiology technicians | Region 1
Region 2 |
1110
541 |
|
| Nurses Professional | Region 1
Region 2 |
191
186 |
|
| Auxiliaries | Region 1
Region 2 |
242
117 |
|
| Administrative | Region 1
Region 2 |
319
42 |
|
| Other personnel | Region 1
Region 2 |
92
21 |
(Note: Piedmont = Region 1, Apulia = Region 2, own elaborations, source: Ministry of Health)
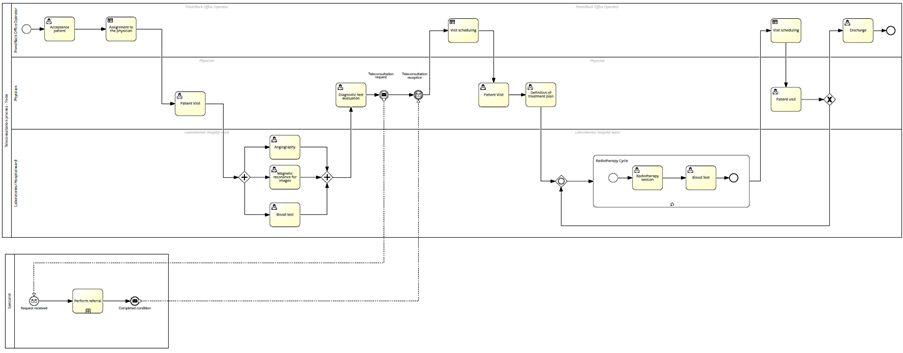
Figure 10 – TO-BE process
Given all the problems that we faced in the process, as from the actual application represented by the log file, we designed a new process aimed at improving this process. Everything is represented in Figure 10.
Related to the AS-IS process, we have improved the TO-BE process in terms of time. In fact, in the TO-BE process modelling, the acceptance and scheduling phases of the visit by the doctor rely on certain decision-making procedures well-defined by the system (based on availability and time of doctors).
The TO-BE process included a change in assigning diagnostic examinations to different technicians in order to optimise the use of resources (personnel and healthcare equipment) and waiting times. Furthermore, as far as the teleconsultation is concerned, we have improved the TO-BE process over the AS-IS process. In particular, in the TO-BE process, the teleconsultation is made automatic both in the phase of specialised doctor identification for a second opinion, and in the consultation requesting phase. Even in the case of sending a second opinion, the TO-BE process is more effective, since it uses the same archiving system, which allows the corresponding doctor to examine the diagnosis in a timely manner.
Moreover, with the TO-BE process, we were able to decrease patients waiting duration and to improve the resources utilization, consequently reducing costs and optimising the healthcare service.
6. Conclusions
This paper demonstrates that process mining is a very-often-used technology in business and industrial processes but can also find useful application in the healthcare sector.
In fact, the process mining tools allow to decrease costs, increase employee and customer satisfaction, and to operate more proactively on a daily basis, which is fundamental in the healthcare sector, where it is crucial to improve the services to patients, especially in terms of care duration and cost reduction (primarily on the management side), taking into consideration the considerable financial commitment required by the sector.
However, although (approximate) data are available to create log files, mostly of them are very personal and not-usable. In fact, due to privacy and confidential reasons, hospital organizations are not disposed to grant or share them.
In conclusion, the application of process mining could make available tools finalised to improve the territorial equalisation of the public intervention (expenditure levels homogenization).
In view of the findings above, it would be suitable to use process mining technique in the health sector, and our hope is that this will take place in the future.
- A. Corallo, M. Lazoi, R. Paiano, F. Striani, “Application of process mining in teleconsultation healthcare: Case study of Puglia hospital. In Proceedings of the 10th International Conference on Information Systems and Technologies”, 1-13, 2020, doi: 10.1145/3447568.3448540.
- W.V.D. Aalst, A. Adriansyah, A.K.A.D. Medeiros, F. Arcieri, T. Baier, T. Blickle, M. Wynn, “Process mining manifesto. In: International conference on business process management”, Springer, Berlin, Heidelberg, 169-194, 2011, doi: 10.1007/978-3-642-28108-2_19.
- W. Van der Aalst, “Process Mining: Overview and Opportunities” ACM Trans. Manag. Inf. Syst., 3, 1–17, 2012, doi: 10.1145/2229156.2229157.
- C.W. Günther, W.M.P. Van der Aalst, “Fuzzy Mining – Adaptive Process Simplification Based on Multi-perspective Metrics”, Lecture Notes in Computer Science, Springer, Berlin, Heidelberg, 4714, 2007, doi: 10.1007/978-3-540-75183-0_24.
- A. Weijters, W. Van der Aalst, A. de Medeiros, “Process Mining with the Heuristics Miner Algorithm”, Technical Report, WP166 Beta Paper Series. Eindhoven University of Technology, Eindhoven, The Netherlands, 2006.
- R. Accorsi, Ernesto D, W. Van Der Aalst, “Unleashing operational process mining”, 2014, doi: 10.4230/DagRep.3.11.154.
- W. Van der Aalst, “Process Mining: Discovery, Conformance and Enhancement of Business Processes”, Springer: Berlin, Germany, Heidelberg, Germany, 2011.
- G. Geleijnse, H. Aklecha, M. Vroling, R. Verhoeven, F.N. Van Erning, P.A. Vissers, X.A. Verbeek, “Using Process Mining to Evaluate Colon Cancer Guideline Adherence with Cancer Registry Data: a Case Study”, 2018.
- C. Fernandez-Llatas, B. Valdivieso, V. Traver, J.M. Benedi, “Using Process Mining for Automatic Support of Clinical Pathways Design”, In Data Mining in Clinical Medicine, Number 1246, Springer: New York, NY, USA, 79-88, 2015, doi: 10.1007/978-1-4939-1985-7_5.
- R. Mans, W. Van der Aalst, R. Vanwersch, “Process Mining in Healthcare”, Springer Briefs in Business Process Management, Springer International Publishing, Cham, Germany, 2015.
- E. Rojas, J. Munoz-Gama, M. Sepúlveda, D. Capurro, “Process mining in healthcare: A literature review”, 61, 224–236, 2016, doi: 10.1016/j.jbi.2016.04.007.
- F. Caron, J. Vanthienen, K. Vanhaecht, E.V. Limbergen, J. de Weerdt, B. Baesens, “Monitoring care processes in the gynecologic oncology department”, Comput. Biol. Med., 44, 88–96, 2014, doi: 10.1016/j.compbiomed.2013.10.015.
- V. Tandon, A. Raheja, S. Mishra, K. Garg, C. Dash, S.A. Borkar, S.S. Kale, “Trends in neurosurgical teleconsultation services across the globe during COVID-19 pandemic”, World Neurosurgery, 150, 2021, doi: 10.1016/j.wneu.2021.03.070.
- P. Baudier, G. Kondrateva, C. Ammi, V. Chang, F. Schiavone, “Patients’ perceptions of teleconsultation during COVID-19: A cross-national study”, Technological Forecasting and Social Change, 163, 120510, 2021, doi: 10.1016/j.techfore.2020.120510.
- P. Baudier, G. Kondrateva, C. Ammi, V. Chang, F. Schiavone, “Digital transformation of healthcare during the COVID-19 pandemic: Patients’ teleconsultation acceptance and trusting beliefs”, Technovation, 102547, 2022, doi: 10.1016/j.technovation.2022.102547.
- C. Fernandez-Llatas, J.M. Benedi, J.M. Garcia-Gomez, V. Traver, “Process Mining for Individualized Behavior Modeling Using Wireless Tracking in Nursing Homes”, Sensors, 13, 15434–15451, 2013, doi: 10.3390/s131115434.
- R. Mans, H. Schonenberg, G. Leonardi, S. Panzarasa, A. Cavallini, S. Quaglini, W. Van der Aalst, “Process mining techniques: An application to stroke care”, Stud. Health Technol. Inf., 136, 573–578, 2008.
- R. Dunkl, K.A. Froschl, W. Grossmann, S. Rinderle-Ma, “Assessing Medical Treatment Compliance Based on Formal Process Modeling”, In Information Quality in E-Health, Number 7058 in Lecture Notes in Computer Science, Springer: Berlin, Germany; Heidelberg, Germany, 533–546, 2011, doi: 10.1007/978-3-642-25364-5_37.
- A. Vathy-Fogarassy, I. Vassányi, I. Kósa, “Multi-level process mining methodology for exploring disease-specific care processes”, 2022, doi: 10.1016/j.jbi.2021.103979.
- D. Gough, S. Oliver, J. Thomas, “An introduction to systematic reviews”, Sage, 2017.
- A. Corallo, M. Lazoi, F. Striani, “Process mining and industrial applications: A systematic literature review”, Knowledge and Process Management, 27(3), 225-233, 2020, doi: 10.1002/kpm.1630 .
- Fluxicon Laboratories, Disco, Available online: https://fluxicon.com/disco/
- M. Egger, G.D. Smith, D.G. Altman, “Systematic reviews in health care: meta-analysis in context”, BMJ Books, London, 2008.
- F. Striani, “Green and Blue Economy: Definitions, Challenges and Limits”, International Journal of Environmental Sustainability and Green Technologies (IJESGT), 11(2), 16-33, 2020, doi: 10.4018/IJESGT.2020070102.
- T. G. Erdogan, A. Tarhan, “Systematic mapping of process mining studies in healthcare”, IEEE, 2018, doi: 10.1109/ACCESS.2018.2831244.
- Z. Valero Ramón, “Dynamic risk models for characterising chronic diseases’ behaviour using process mining techniques”, Doctoral dissertation, Universitat Politècnica de València, 2022, doi: 10.4995/Thesis/10251/181652.
- M. Weske, “Business process management architectures – Third edition”, Springer, Berlin, Heidelberg, 2019.
- D. Bano, J. Michael, B. Rumpe, S. Varga, M. Weske, “Process-aware digital twin cockpit synthesis from event logs”, Journal of Computer Languages, 101121, 2022, doi: 10.1016/j.cola.2022.101121.
- M. Dumas, M. La Rosa, J. Mendling, H.A. Reijers, “Introduction to business process management”, In Fundamentals of business process management, Springer, Berlin, Heidelberg, 1-33, 2018, doi: 10.1007/978-3-662-56509-4_1.
- M. Ramos-Merino, L.M. Álvarez-Sabucedo, J. M. Santos-Gago, J. Sanz-Valero, “A BPMN based notation for the representation of workflows in hospital protocols”, Journal of medical systems, 42(10), 1-10, 2018, doi: 10.1007/s10916-018-1034-2.